


{kind=link}
The prospect of HPE raises profound ethical challenges. One significant concern is that HPE will lead to renewed interest in eugenics3. The eugenics movement arose in Victorian Britain aiming to ‘improve’ the gene pool of future generations, essentially by advocating government policies that would lead to people such as those in the movement leaving more offspring31. This kind of eugenics has been termed ‘positive eugenics’31. Other countries adopted ‘negative eugenics’ policies, which imposed severe, unethical restrictions on peoples’ individual liberties (for example, forced sterilization) to prevent those considered to have ‘undesirable’ genes from reproducing31. Intellectual disability, psychiatric diseases, criminality and poverty were targets of the eugenics movement in Germany, other parts of Europe, Canada, Australia and the USA from the late 19th century to the early 20th century. Nazi eugenics was based on race and included systematic mass murder at an unprecedented scale, forced sterilization and other human rights abuses. Could HPE lead to a 21st century reincarnation of previous eugenics practices? Potentially, if it is used by non-democratic state actors, such as those that already adopt coercive control over populations.
To ensure that future uses of HPE are not eugenic, it is crucial to emphasize respect for individual liberty and societal values, such as diversity, equality and non-discrimination. A state should neither impose its vision of a good life on individuals nor use coercive measures to encourage the use of HPE. Similarly, the practice of reducing the incidence of a disease should not be equated with the notion that having a disease affects an individual’s inherent moral worth. Rather, we propose that any future use of HPE should be modelled on modern clinical genetics, which uses genetic technologies to further the goals of medicine. In democratic societies, clinical genetics is voluntary and based on non-directive counselling, provision of information and choice, and interventions aimed at the well-being of the future child. When implemented with appropriate regulation and governance, HPE can be distinguished from past eugenic practices, as in contemporary clinical genetics.
Nevertheless, even if used within democratic health systems and modelled in clinical genetics, HPE may lead to undesirable outcomes for individuals and society. Since the 1970s, philosophers and bioethicists have been debating the ethical implications of altering our genetic makeup using biotechnologies32,33,34. We highlight the major ethical arguments in favour and against HPE in Table 1 from these debates2,3,21,35,36,37,38,39,40,41,42,43,44,45,46. The modelling we have done has direct implications for three ethical issues related to HPE (that is, ‘enhancement’, inequality and diversity).
Gene editing for non-disease traits
The same techniques that enable HPE to reduce the risk of diseases can also be used to alter non-disease traits, including physical attributes, personality and cognitive traits. Using genetic technologies for purposes other than treating diseases, sometimes referred to as enhancement in the bioethics literature47, raises specific ethical concerns. We note that human enhancement is a highly contested term, and more neutral phrasing, such as ‘change of non-disease traits’, may be preferable. It is sometimes assumed that to genetically change human non-disease traits, new genetic material would need to be incorporated into the genome42. Our modelling challenges this assumption. It indicates that HPE could lead to human phenotypes that have never been previously observed and are many standard deviations from the current mean (Fig. 1). It is conceivable, at some point in the future, that HPE could be used to target traits, such as height and intelligence, and lead to large-scale changes in these traits. Although human populations have undergone dramatic changes over the past few generations as a result of cultural and environmental changes, the prospect of radical, rapid changes in human physiology raises unique ethical concerns48. Future populations with radically different physiologies and psychologies may develop very different values from those living today. Human change in non-disease traits could change society in unprecedented ways and not necessarily for the better. Furthermore, using HPE to make individuals ‘better than well’49 can be seen as unfair in a world where many people do not have access to adequate healthcare.
It is currently possible to test embryos created through in vitro fertilization for their predisposition to non-disease traits. However, many jurisdictions only allow embryos to undergo genetic testing and screening to prevent a serious disease50. Nevertheless, when considering polygenic traits, the line between health and disease is blurred5. For example, is using HPE to reduce blood pressure, a causal risk factor for common diseases, a medical or non-medical application? The same question arises regarding vaccines and other preventative interventions. In extreme cases, polygenic editing can be used to delay normal human ageing, significantly prolonging human life.
One approach could be to limit the use of HPE to cases in which there is a reliable relationship between a trait and positive effects on well-being51. Of course, this raises the vexed issue of which conception of well-being to use, but this is a problem for any welfarist approach to individual or societal improvement.
Another possibility is to limit HPE to combinations of protective alleles that naturally occur in today’s populations. Some people alive today possess great genetic resistance to polygenic diseases. For example, the chance of an individual carrying ten protective alleles against AD (thus having a risk of 0.3%) is one per two billion, indicating that there may be people alive today with this combination. Similarly, there may be people alive today who enjoy genetic protection against a wide range of polygenic diseases. These already existing combinations of protective variants could be the targets of HPE. In such cases, the goal is to provide protection to those in a population with the highest risk of developing a polygenic disease, similar to those with the lowest genetic risk. This would be egalitarian and promote genetic equity, where HPE could be used to make people as healthy as the healthiest people living today.
Data on public attitudes towards genome editing suggest other concerns. While most countries are strongly against using gene editing technology to increase intelligence, others are not. A recent study analysing public attitudes towards genome editing around the world found one country outlier regarding support for targeting non-disease traits. In India, 64% of respondents were in favour of germline editing and intelligence—far higher than in any other country surveyed52. A recent survey of 6,800 people in the USA reported that about 40% of respondents deemed heritable gene editing for medical and non-medical traits either ‘not a moral issue’ or ‘morally acceptable’53, and only 17% believed it was wrong. If HPE becomes a possibility, perhaps we should consider a future where HPE is restricted in some countries but unrestricted in others. Countries might feel pressure to allow HPE for non-disease traits out of fear of being outcompeted by countries that embrace the technology.
Inequality
An enduring concern regarding genetic and other technologies is that they will increase inequalities, making the dominant social class the dominant biological class, as depicted in the film Gattaca54. Although many technologies are initially only accessible to those that can afford them, there is reason to be concerned about differential access to HPE. Inequalities in wealth are substantially social in nature, reflecting unequal access to resources and opportunities, which can be corrected. HPE could write these inequalities into our biology.
Our modelling gives substance to these concerns by showing that dramatic changes can be achieved through HPE. Individuals with edited genomes may have a much lower risk of disease than those with unedited genomes. If HPE is only available to those in higher socio-economic groups, then this will more heavily skew the disease burden of polygenic diseases to those who are already the worst off55. Diseases such as depression and heart disease may become diseases that only occur in certain demographics.
The unequal use of HPE is likely to increase social division. In Fig. 3, we quantify the increase in inequality of the risk of diseases as a function of the proportion of the population undergoing HPE. Additional results for several hypothetical diseases are also given in Supplementary Fig. 4. These results show that there is an increase in inequality, as measured by the Gini index, when a small proportion of the population carries edited genomes and that inequality is only decreased when more than 50% of the population has edited genomes.
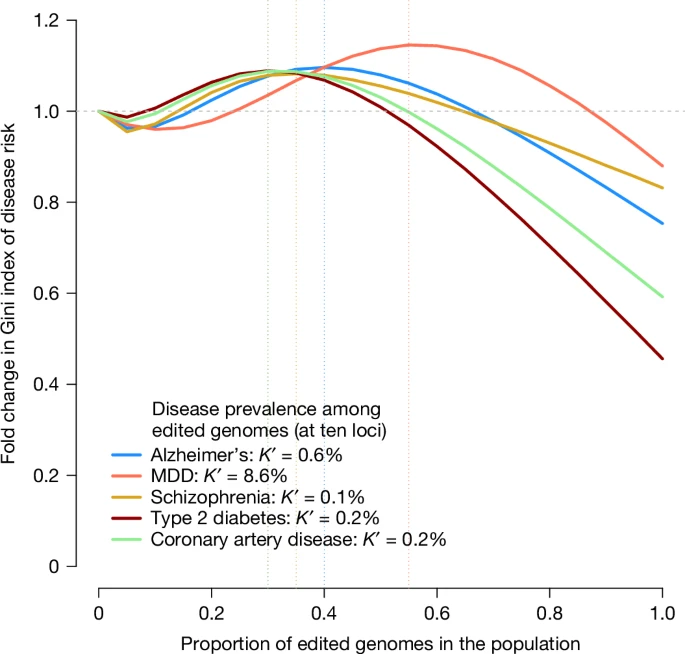
We modelled the probability of disease in the population as a mixture distribution with two components: one component with a reduced risk, representing the fraction of edited genomes in the population, and another component representing unedited genomes (Methods). Diseases and prevalence among non-edited genomes are the same as those shown in Fig. 1. The prevalence among edited genomes (K′) was taken from Fig. 1, assuming ten edited loci. The x axis represents the fraction of edited genomes in the population, varying from 0 to 1, and the y axis represents the relative Gini index in the population compared to a population with no edited genomes. The vertical dotted lines indicate which fraction of edited genomes in the population yields the maximum Gini index for each disease (that is, maximum risk inequality). The source code used to generate the figure is provided in ‘Code availability’.
Existing genetic variations contribute to social and health inequalities. For example, people with more alleles associated with higher educational attainment are more likely to migrate to locations with better economic opportunities. This leads to an increase in social stratification56, which, when combined with the common practice of assortative mating on traits associated with educational attainment, can increase the phenotypic variation in the population by as much as 20% (ref. 57), thereby increasing health inequalities for common diseases genetically correlated with educational attainment. Reducing health inequalities caused by a random genetic lottery58 seems fair and desirable. Providing equitable access to new technologies, such as GWAS and their downstream clinical translations today59 and, perhaps, HPE in the future, could reduce health inequalities.
Reducing the incidence of polygenic diseases could further lead to a more equitable distribution of health resources within health systems. Common chronic diseases, such as heart disease and psychiatric disorders, are the main contributors to the global cost of healthcare and contribute substantially to the loss of disability-adjusted life years. Reducing the amount of health resources spent on fighting these diseases could free up resources that could be reinvested in other health priorities. Reducing the number of people whose health depends on access to resources will free up resources for others in need.
The implications of international inequality may be more difficult to control. However, many countries are unlikely to have the capacity to use HPE. If high-income countries use HPE, this could result in polygenic diseases becoming even more concentrated in developing countries.
There are no easy solutions to these problems, which is why it is vital that we start to consider the implications now while the prospect of HPE is still many years away.
Diversity
One concern in human genetic engineering is that this will lead to a loss of genetic diversity60,61. Examples of the dangers of a lack of genetic diversity are found in agriculture. Modern crops have been selected for their enhanced efficiency in food production but tend to be more susceptible to disease epidemics and have a reduced capacity to adapt to changes in environmental conditions. Similar concerns have been expressed regarding the use of heritable gene editing in humans. In the pursuit of healthy, happy children, there is fear that we might create genetically homogeneous human populations with increased susceptibility to disease and decreased potential for adaptation to future risks61. However, our modelling suggests that these concerns are mostly unfounded for HPE. For the traits considered, there was a high degree of background genetic diversity, with tens of thousands of loci responsible for the observed genetic variation. Relatively few genetic changes are needed to make very large changes to phenotypes and reduce disease risks. This suggests that it is possible to radically reduce the risk of polygenic diseases in human populations while maintaining high levels of genetic diversity. Moreover, modern approaches to disease prevention and treatment, such as the human immunodeficiency virus and Covid-19 pandemics, do not rely on genetic diversity and resilience, but on the application of science to develop therapeutic and biopsychosocial interventions to manage disease. Indeed, HPE or somatic gene editing can, in theory, be applied to confer genetic resistance.
A collectivist ethical approach
The use of genome editing technologies by individuals and couples will affect individuals’ genomes, which will affect their whole lives in multiple ways, as well as the human gene pool. This will require a holistic evaluation of the effect on a whole life that requires a benchmark of a good human life, which is a topic of thousands of years of philosophical debate. However, this also suggests that there may be limitations to ethical approaches to HPE that focus solely on its effect on individuals.
One alternative ethical perspective is based on collective welfarism. According to this approach, the goal of biotechnology should be to provide benefits to individuals and to broader groups of individuals, including families, communities and societies4. From this perspective, it is also important that HPE not be implemented in ways that decrease social cohesion, increase division and weaken our communities and society. Notably, this approach requires further analysis of what constitutes flourishing societies.
In the long term, there may be an obligation to pursue and develop technologies such as HPE. Mildly deleterious mutations that escape natural selection because of better medical care are predicted to accumulate in the gene pool62. Previously published models suggest that the effect of this ‘genetic load’ might manifest itself as physical and mental deterioration in only a few generations62. However, this concept is controversial, and the conclusions are debated63,64,65. If we take seriously the idea of leaving future generations in a better state than the current generations, then we have reason to provide them with the preconditions for a good life. This includes access to clean water, unpolluted air, education and shelter, and may include the use of HPE to lower the genetic risk of disease.
Although collectivist considerations should inform the values of governments and the goals they pursue, it is also important that these goals do not override basic human rights, such as the right to autonomy. The pursuit of collectivist goals must be compatible with basic human rights.