


{kind=link}
Japan is brimming with signs of an approaching medical revolution. Shiny white robots are tending dishes of cells, rows of incubators hum in new facilities, and a deluxe, plush-carpeted hospital is getting ready to welcome its first patients.
Building on the Nobel-prizewinning work of stem-cell scientist Shinya Yamanaka, researchers across the country are crafting cells into strips of retina, sheets of cardiac muscle or blobs of neurons, in the hope of treating blindness, mending hearts and reversing neurodegeneration. Results from early-stage clinical trials — some announced just in the past few weeks — suggest that the cells might actually be working to treat conditions as varied as Parkinson’s disease and spinal-cord injury.
‘Big leap’ for Parkinson’s treatment: symptoms improve in stem-cells trials
Now, after nearly two decades of hard work and setbacks, many say that Japan is on the cusp of bringing these therapies to market.
Yamanaka, who runs a lab at Kyoto University, discovered in 2006 that adult cells could be reprogrammed into an embryonic-like state, capable of becoming practically any kind of tissue1. These induced pluripotent stem cells — or iPS cells — won Yamanaka the Nobel Prize in Physiology or Medicine in 2012, and propelled him to superstar status. They have become a symbol of the country’s global scientific aspirations.
The Japanese government has poured more than ¥110 billion (US$760 million today) into research and development on regenerative medicine, on top of billions more from private funders, organizations and companies. “People thought, ‘Now we can treat any incurable disease’,” says Shigeto Shimmura, director of Fujita Health University Haneda Clinic. “There was so much hype.”
Scientists launched clinical trials and start-up firms. Large biotech companies swooped in, investing even more in manufacturing hubs. Now, medical facilities are preparing to welcome a rush of patients from Japan and abroad. “Regenerative medicine in Japan is moving very dramatically,” says Masayo Takahashi, an ophthalmologist at Kobe City Eye Hospital and president of the biotechnology company, Vision Care. In 2014, she became the first to treat someone with cells derived from iPS cells.

Masayo Takahashi ran the first clinical trials for iPS cells.Credit: Ben Weller for Nature
There are more than 60 iPS-cell clinical trials in progress worldwide, nearly one-third of them in Japan. The treatments have proved to be safe and shown signs of benefit. Moreover, the technology has been improving apace, says Shimmura. And thanks to a fast-track approvals process for regenerative medicine, Japan could become the first country to approve iPS-cell-based treatments. This could happen within a year for Parkinson’s disease.
But those approvals are not yet in hand, treatment costs are high, large trials showing clear clinical benefit have yet to materialize, and concerns about safety could still sap the public’s willingness to try this treatment. “We’re down to realizing what the potential of these cells are, and what the limits are,” Shimmura says.
Eye see
Yamanaka’s iPS cells promised to bypass a bioethical stand-off that had threatened the potential of embryonic stem cells for a decade. Because production of iPS cells doesn’t require the destruction of human embryos, they were considered ethically less fraught. Furthermore, because they could be made from the cells of the person in need of treatment, they promised to offer transplantable tissues without the need for immune-suppressing drugs.
In 2014, Takahashi put this idea to the test. She took skin cells from a 70-year-old woman with a progressive eye condition known as macular degeneration and guided them into a younger, more pliable state using a recipe similar to the one Yamanaka had devised and refined. The resulting iPS cells were then grown into thin sheets of retinal cells and transplanted into the woman’s eye, where they have survived for ten years and prevented further vision loss, Takahashi says.
It was a procedure with practical limitations, however. Self-derived, or ‘autologous’, cell therapies are time-consuming and expensive to make, and the large cell-sheets that researchers crafted for implantation required intrusive surgery. Takahashi says she chose this approach to ensure the highest chance of clinical benefit — to demonstrate to the world what was possible. It was designed to be “scientifically, the best treatment”.

A technician at Vision Care in Kobe makes capillary tubes for injecting cells into the eye.Credit: Ben Weller for Nature
But Takahashi wanted to create a commercially viable treatment. This meant a change in approach, using cells from donors that could be mass-produced, and finding less invasive ways of getting them into the eye.
She and her team initially tried injecting a pool of donor-derived cells just under the retina, where they might form sheets on their own. But the researchers had limited control over where the cells grew. They next tried growing strips of cells, 2 centimetres long and 200 micrometres thick. They used a tube to slide several of these strips onto the retina through a tiny incision in the eye, in the hope that they would expand into sheets.
Don’t rush promising stem-cell therapies
Results published in March suggest that for three individuals who received the treatment, the cells have survived and are safe one year after surgery2. But the signs of benefit are mixed. One of the three individuals said she could see her husband’s face clearly for the first time in ten years, but only through a small section of her eye, where the cells had been transplanted.
The difficulties might come down to the retina’s natural resistance to regeneration. But other parts of the eye might benefit more from cell therapies: the cornea, the clear covering that lets light in, is maintained by a pool of stem cells and constantly being rebuilt.
In November, Kohji Nishida, an ophthalmologist at Osaka University, and his colleagues published the results of donor iPS-cell-derived transplants into four individuals for whom those natural cornea-building stem cells had been depleted — a condition that results in corneal scarring and vision impairment. Three of them saw sustained gains in vision3.
Nishida has since set up a start-up company, Raymei, which plans to launch a larger trial and aims to gain formal approval in three years. “The next clinical trial is pivotal,” he says.
Brain and back
The regeneration of nerve tissue has been one of the great hopes for iPS cells, but it has been fraught with challenges. Jun Takahashi, husband to Masayo, has an office lined with statues of elephants and an imposing, life-sized set of navy-blue samurai armour, “just to encourage my lab”, he says.
Takahashi is a neurosurgeon and the director of Kyoto University’s Center for iPS Cell Research and Application (CiRA), an institute established by Yamanaka as a hub for iPS-cell research.

Jun Takahashi is trying to treat Parkinson’s.Credit: Ben Weller for Nature
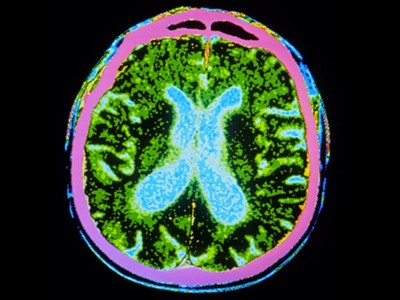
In 2018, Takahashi led a trial that used donor-derived iPS cells to treat Parkinson’s disease, a degenerative brain condition that affects movement. The team injected between five million and ten million cells, which had been coaxed into acting like neural progenitors, into the right and left brain hemispheres of seven individuals with the disorder.
Two years after the treatment, according to results published this week, at least four individuals saw noticeable improvements in symptoms, such as fewer tremors and rigid movements4. One went from requiring assistance to being able to live independently when not taking their regular medications. Another trial involving 12 individuals using neural progenitors derived from embryonic stem cells also showed, on average, moderate improvements in movement 18 months after the transplant5. Knowing that the treatment could work has brought Takahashi great relief.
Paralysed man stands again after receiving ‘reprogrammed’ stem cells
But, unlike his wife, he has not set up a company to develop the technology for manufacturing the cells and conducting the surgery. Instead, he has instead transferred that knowledge to Sumitomo Pharma, based in Osaka. “As a scientist, I am kind of satisfied,” he says. He has now diverted his attention to developing cell therapies for treating stroke.
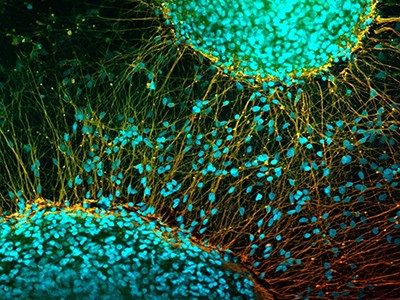
Hideyuki Okano, a stem-cell scientist at Keio University in Tokyo, has demonstrated another potential trick for iPS cells. Between 2019 and 2023, he and his colleagues used donor-derived cells to treat four people with spinal-cord injury. The researchers presented preliminary results — not yet peer reviewed — at a press conference in March, showing that one individual with paralysis can now stand independently and is learning to walk. Another can move some of their arm and leg muscles but cannot stand. Two others did not show substantial improvements.
Similar trials are under way outside Japan, some of which involve many more participants than the Japanese trials. But unlike other regions, Japan has made the path to approval relatively easy, says Clive Svendsen, a stem-cell researcher at Cedars-Sinai Medical Center in Los Angeles, California. In 2013, Japan introduced a system through which regenerative-medicine products could be conditionally approved if they are shown to have no major safety issues and are likely to be efficacious.

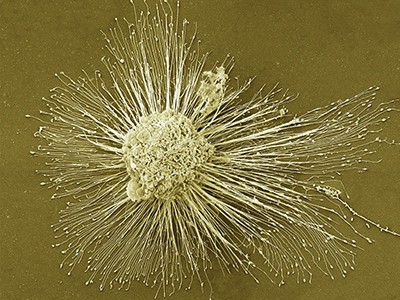
Jun Takahashi and a colleague examine a cluster of nerve tissue created from iPS cells (shown magnified on the right).Credit: Ben Weller for Nature
Companies can offer the treatments, with costs mostly covered by the national health system. But they must continue to collect data on safety and efficacy to earn full clinical approval.
Some researchers have raised concerns about this fast-track process and related programmes in Japan. Last year, two of the four products that had received conditional approval under this mechanism — one involving thigh-muscle cell transplants for the heart, the other a gene therapy to treat ulcers in narrowed arteries in the limbs — were withdrawn. The first was rejected for formal approval after nearly a decade on the market because it failed to show clinical benefit. The second was withdrawn about five years after being conditionally approved, because surveillance data did not reproduce results observed in earlier trials.
Hiroshi Kawaguchi, an orthopaedic surgeon at Nadogaya Hospital in Kashiwa, says he is concerned that the fast-track process shifts the cost burden from pharmaceutical companies, which would otherwise have to conduct large-scale trials, to the public insurers, which then pay for expensive, unproven treatments. Last year, Japan’s Ministry of Health, Labour and Welfare issued guidance documents that clarified that conditional approval should not be the ultimate goal for companies.
Others are less concerned about Japan’s fast-track process for conditions that are rare or have few other treatment options. “In order to move this field forward quickly, you’re going to have to have an element of risk,” says Svendsen. “What I’ve seen in Japan has been pretty sensible; they are putting regulations in place.”
iPS cells for all
Even without approvals in hand, the industry is building capacity in the expectation that demand for these treatments will be high. In 2018, Sumitomo Pharma completed construction of what it describes as the world’s first manufacturing facility for donor-derived iPS-cell products. The building, in Osaka, looks like a giant, floating silver box. In 2020, it delivered its first cells for transplant — for the fourth participant in Takahashi’s Parkinson’s trial. The company is also supporting two early-stage Parkinson’s trials in the United States.
Masayo Takahashi has chosen a more portable manufacturing model for her macular-degeneration treatments: a white, muscular-looking, two-armed robot. Powered by machine learning, it checks in on cells’ progress as they are prepared for transplant through a microscope. In 4 months, it can produce enough cells for more than 800 individual treatments.

This robot in Kobe is preparing cells for transplant to treat people with macular degeneration.Credit: Ben Weller for Nature